
A report on an ERZ controller trapped in an airlock door during an inspection of final seals and gas monitoring stations in return airways has highlighted issues around effective working alone procedures and processes. The Queensland Department of Natural Resources and Mines has recently released the investigation report urging mines to review current practices around working alone among a range of other hazards.
The Department confirmed that a mine ERZ Controller sustained permanent disabling injuries after his leg was trapped in an airlock door for over five hours. This potentially life-threatening injury also had a high risk of amputation.
It also follows another USA based incident where a mineworker was killed in auto closing doors.
How did the incident occur?
Background of the incident
Workers at a central Queensland mine were monitoring a longwall seal up process, part of which included regularly inspecting the final seals and gas monitoring stations in the return airways.
While accessing a return airway to conduct bag sampling, an ERZ Controller became trapped at a portal airlock entrance—one of five portal airlock entrances along a high wall.
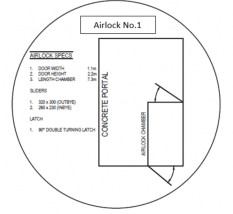
Of the five portal airlock entrances at the site, three were of different designs.
Airlock 1 (see image 1) is the design of the airlock the ERZ Controller was trapped in at the outbye door.
![]()

 Airlock 2 is a common airlock design normally used for access at points with high-pressure differentials.
Airlock 2 is a common airlock design normally used for access at points with high-pressure differentials.
A third design (not shown) had both doors opening toward the return airway (inbye). The mine had no established standard for airlock design at the time of the serious accident.
At the time of the serious accident, up to 1981pa pressure differential appeared across the airlock where the serious injury occurred, calculated to produce 426.4kg force against the ERZ Controller’s leg.
The site did have a current procedure for ‘Working alone in isolated areas’ (‘working alone’ procedure) of the mine, however, the procedure was not applied and monitored consistently.
The same mine had a serious accident in 2013 when a coal mine worker was trapped in a cable reeler on the surface of the mine. In similar circumstances, the injured worker was not found immediately and sustained a permanently disabling injury.
This incident was the impetus for implementing the ‘Working alone’ procedure at the mine.
Investigation of the incident
When the ERZ controller began to open the outbye door he stepped into the doorway of the airlock to push the door further open. As this occurred the inbye door of the airlock swung open, short-circuiting the ventilation and causing the outbye door to slam closed, trapping the ERZ controller by the leg.
The investigation identified the mechanism for the inbye door opening was the brattice covering the inbye door shifting, as the change in pressure against it increased, and that the inbye door handle had been modified during a repair and could no longer fully latch closed.
It is plausible that the brattice shifting rapidly, the lesser area of the handle contacting the door frame and the high-pressure differential, all contributed to the uncontrolled opening of the inbye door.
The ERZ Controller was trapped by the inbye door for over five hours. The ‘working alone’ procedure wasn’t used by either the ERZ Controller or the control room officer for this task on this day. About two hours into the following shift, the ERZ Controller was found by coal mine workers, who were in the vicinity gathering timber for an unrelated task.
An alert had been raised for the ERZ Controller’s whereabouts prior to this, but this alert had not escalated beyond checking tag boards, lamp racks and verification phone calls to employees’ listed contacts.
Key issues
Findings from the nature and cause investigation
- There was a failure to maintain an acceptable level of risk in the workplace.
- Design of the airlock itself was fundamentally incorrect for the purpose of providing safe access from intake to return airways with a high-pressure differential.
- None of the mine statutory officials interviewed identified the airlock design as a hazard prior to the incident.
- High-pressure differential risk at airlocks was identified in planning meetings up to seven years prior to the serious accident occurring. There was no record or evidence of this being actioned.
- There was no evidence that the change management process was applied when the airlock design was modified; nor was there evidence of a risk assessment being conducted for the original airlock design.
- The scope of work for the design and manufacturing of the airlock did not identify how the airlock was to be constructed, the location of doors or how they were to be operated.
- Installation inspections and checklists were not applied for the airlock involved in the serious accident.
- Hazard reports previously identified the risk of high-pressure differential and airlock doors swinging in the wrong direction. Actions applied did not deal with the hazard identified.
- The ‘working alone’ procedure implemented in 2013 had not been enforced fully at the mine.
- Mine statutory officials had a poor understanding of the ‘working alone’ procedure at the time of the serious accident.
- Sixty-six days prior to the serious injury, a ‘Field Leadership’ audit by a senior management team member found deficiencies in applying the ‘working alone’ procedure. Actions raised from this audit weren’t implemented at the time of the serious accident.
- Some coal mine workers at the site (including the injured ERZ Controller) hadn’t received ‘working alone’ procedure training.
- None of the statutory officials interviewed could accurately identify what constitutes an abnormal change in the mine’s main fan pressure and the trigger point for an alarm in the control room.
- As part of its investigation, the Queensland Mines Inspectorate reviewed 179 statutory reports dating back 6 months before the serious injury. These reports identified that statutory officials had regularly used the same airlock where the serious injury occurred. Fourteen of these reports were found to have comments identifying ventilation control device design hazards and pressure differential risks. There was a less than adequate response to address the risk. Of the other 165 inspection reports referencing access through the airlock, statutory officials failed to identify any hazard or risk associated with the airlock.
- An IMAC gas monitoring station next to the portal was alarming due to low oxygen detected at the sensor return side of the seal. The alarm was disabled in Safegas as it was deemed no longer required and so did not alarm at the control room. Had the alarm sounded in the control room and another ERZ Controller been sent to investigate, the trapped ERZ Controller would have been found much sooner.
- Evidence of a lack of line of control/management by the mine in implementing corrective actions for hazardous conditions recorded on statutory reports and hazard reports.
Recommendations to improve health and safety
- Ensure Safety and Health Management System (SHMS) Effectiveness Audits are conducted, reviewed and corrective actions implemented. S41, 62(5)(f), CMSHA 1999.
- Ensure training in SHMS procedures is conducted and recorded. S82 & 84, CMSHR 2017.
- Ensure actions identified from site audits and inspections are actioned with an urgency applicable to the residual risk. S30, CMSHA 1999.
- Ensure all Coal Mine Workers are aware of their obligations under the CMSHA 1999 and the SHMS. S39 & 42, CMSHA 1999.
- Ensure a system is in place for dealing with hazards identified in statutory reports. S98, CMSHR 2017.
- Ventilation Officers shall:
- ensure adequate ventilation of the mine
- ensure the mine’s air quality is measured and recorded
- take charge of any ventilation system change in the mine by giving directions, or by being present when the change is happening,
ensure all ventilation control devices (VCDs) at the mine are properly constructed and maintained.
- To achieve an acceptable level of risk, the Ventilation Officer shall also monitor and record pressure differentials across VCDs throughout the mine. This must take into account, as a minimum, the proximity of the VCD, rating of the VCD, access required through the VCD and why, size and weight of the doorway and history of injuries to persons caught in ‘Man access’ and or ‘Machine access’ doors. From this information, it is recommended the Ventilation Officer establish a baseline pressure/standard to apply when an airlock is required due to an excessive pressure differential. S341, S351 CMSHR 2017, S30 CMSHA 1999.
- It is recommended Ventilation Officers establish standards for airlock design for their mine. S341(d), S350 CMSHR 2017. S30, S38, S44 CMSHA 1999.
- Audit compliance to procedures, forms and processes for changing gas monitoring equipment locations or changing/disabling alarms. S223 & S224 CMSHR 2017.
- Assess the risk to coal mine workers for working alone throughout the mine, both surface and underground. S30 & 38 CMSHA 1999.
References and further information
Safety News Flash ERZ Controller leg caught in an access door of an Airlock. (24 April 2017)
Mine Safety Alert no.127 Ventilation control devices. (21 May 2005 Version 1.)
Coal Mine Safety and Health Act 1999 (CMSHA 1999).
Coal Mine Safety and Health Regulation 2017 (CMSHR 2017).
The report was first published by the Queensland Department of Natural Resources & Mines as Mine ERZ Controller sustains injuries trapped by an airlock door Mines safety bulletin no. 180 | 14 March 2019 | Version 1. Mines are urged to share the information.
Read more Mining Safety News











Add Comment